Free Courses Sale ends Soon, Get It Now
Free Courses Sale ends Soon, Get It Now

Disclaimer: Copyright infringement not intended.
Context: Union Health & Family Welfare Minister Mansukh Mandaviya declared that India is committed to eradicating Lymphatic Filariasis by 2027, surpassing the global target by three years.
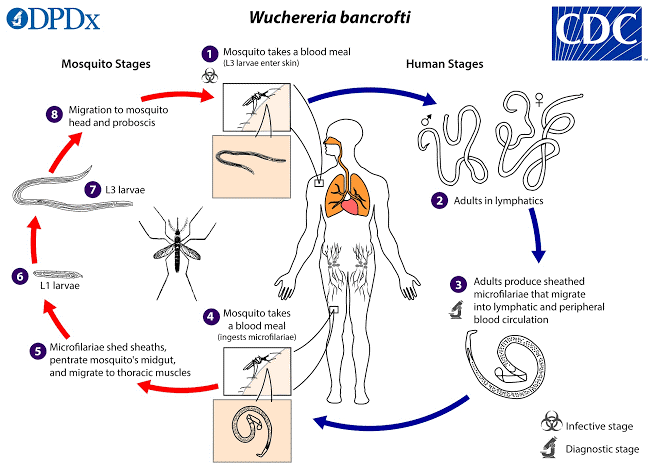
Lymphatic Filariasis
Etiology
Epidemiology

Trend and present endemicity of filariasis in India
Pathophysiology
Main challenge
Filariasis Control in India
Way ahead
Conclusion
|
PRACTICE QUESTION Q. India is committed to eliminating Lymphatic Filariasis by 2027, three years ahead of the global target. However, the road to achieve the target is tough and multiplicity of efforts are required. Critically analyze.(250 Words) |
.jpg)
© 2024 iasgyan. All right reserved