Free Courses Sale ends Soon, Get It Now
Free Courses Sale ends Soon, Get It Now

Copyright infringement not intended
Context: The Rajasthan Assembly's recently completed budget session restarted discussion about the Right to Health Bill.
Details
.jpeg)
Key points of the Bill
Concern
|
Right to health under the Indian Constitution ● The right to health is not specifically mentioned in the Indian Constitution. The theoretical "right to health" is drawn from the constitutionally protected rights to life and liberty (Article 21). ● In the past, courts have underlined the State's duty to safeguard and advance citizens' health, citing constitutional clauses like Article 38 (promotes the welfare of people) and Article 47 (directs the government to meet the population's nutritional and health needs). |

State of India’s healthcare sector
How much does India spend on healthcare?
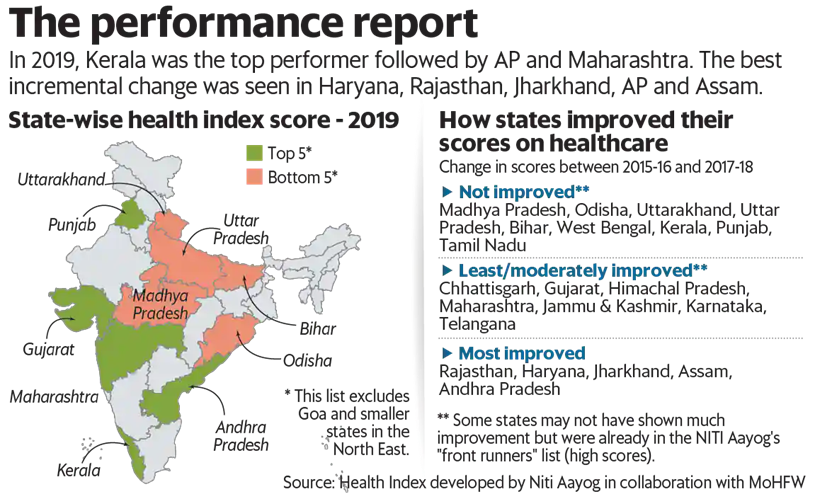
How do states rank on the health index?
Problems with Health Care Infrastructure of India:
Shortage of Staff and Equipment
Inter-State and Intra-state variations
No proper regulatory mechanism and monitoring
Lack of Affordability:
Way forward:
|
PRACTICE QUESTION Q. Examine the issues that the Indian healthcare system is experiencing and make suggestions to raise the standard and accessibility of healthcare in the nation. |
© 2024 iasgyan. All right reserved
{kind=link}